Between 25 and 40 percent of Americans with mental illnesses will face incarceration in their lifetime, according to the National Alliance for Mental Illness (NAMI).
Twenty five to forty percent.
Just by inheriting, being born with, or developing a chemical imbalance in your brain, you are put at severe risk of spending the majority of your life behind bars. Or, if you are lucky enough to escape the repetitive cycle of street life to jail time to life on the street once again, you will still be permanently branded with a criminal label practically tattooed to your forehead, screaming “I am unsafe to be around” to any future employer or partner.
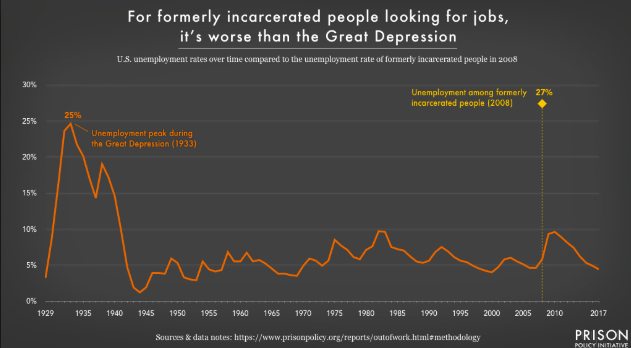
Photo courtesy of PRISON Policy Initiative.
Two questions naturally arise: Are these mentally ill “criminals”, who might justifiably be labeled patients, really bad people; and, how is this cycle fair?
Although the American incarceration process is complex, these answers are quite simple. No, the mentally ill cannot unfairly be defined by a mistake that was completely out of their conscious control, and, it plainly isn’t fair.
Incarceration of the mentally ill has been a long-standing issue governing American politics, criminology, and mental-health movements for decades, and however many tactics are used to attempt to gain momentum to improve, little has seemed to stick. In recent years, though, hope springs again, as a new program providing complete community partnership on all fronts has shown some promising growth in how the cases involving the mentally ill are handled.
NAMI’s explanation of CIT programs.
Crisis Intervention Teams (CIT) are programs that work to provide training from professionals in the psychiatry and psychology fields to first-responding police officers. NAMI states that more than 2,700 communities nationwide have implemented this strategy as of today. Outlined by NAMI are the main benefits of CIT programs, including the fact that “diversion programs like CIT reduce arrests of people with mental illness while simultaneously increasing the likelihood that individuals will receive mental health services”. CIT programs aid police officers in learning precise procedures to carry out when dealing with a suspect who they consider mentally ill in the heat of crime or confrontation. This way, instead of rashly killing the suspect, or taking them into the revolving doors of American prisons, the suspect can be taken directly to a treatment center to get the medical attention they need.
The medical attention that should be customary, a human right, for the mentally ill.
Because although the mentally ill suspects are often perpetrators of their crime, they are simultaneously victims of their mind.


Journalist Pete Earley discusses this topic in his research- and experience-based novel, Crazy. Earley roots his passion for aiding the mental-health incarceration crisis in his role as a father of a bipolar son, who broke into and entered a random house during one of his delusional episodes. Earley quotes Armstrong, a prosecutor who advocates for the mentally ill on trial, “Most of the mentally ill defendants whom we deal with are not criminals. They didn’t have any concept of what they were doing when they committed a crime. If the point of prison is punishment and rehabilitation, then what are these people being rehabilitated from—their mental illness?” (311). The point of highlighting the mental illness of an accused is not to excuse their dangerous (unconscious) behavior, because it does put others in the community at risk, especially when dealing with major crimes. Rather, the point is to emphasize that the mentally ill should not even be given the opportunity to put others at risk by being cycled between jails and streets, and should instead be put in treatment. This is where Crisis Intervention Teams come in, giving police the tools and skills to intervene at a front-line level, and prevent mental ill incarceration from growing exponentially, creating an ever-expanding or ever-repetitive cycle.
As nice as it would be to say that the idea for CIT programs arose solely from a desire for change, unfortunately it is not the truth. The creation of the program was a reactive measure, formed after a tragic shooting in Miami. Randy Carlos Baker, a 49-year-old black man, was walking home from his cousins’ house while a bank robbery simultaneously occurred a few blocks down. Out of racial profiling, a Miami police officer pulled up next to Baker, who insisted he had done nothing wrong. Due to Baker’s mental illness, he became aggressively angry. A fight followed as more police officers were brought in as backup, and it ended with a three bullets in Baker’s now-dead body.
Again, Baker had done nothing wrong, yet his family was now mourning his loss, and he would never make it to age 50.
Earley writes about how Miami Herald columnist Jim DeFede emphasized in his work, “‘Baker did not have a criminal record and had not broken any laws when the police decided to question him. ‘Randy Baker’ should be alive today’ he declared. […] DeFede noted that nearly all thirty-four municipalities in the county that had operated their own police departments had added CIT training—except Alvarez’s [the department in which Baker was shot]” (348). Innocent people are being shot due to a mix of their target social identities: not only was Baker mentally ill without receiving proper treatment, but he was also black, predisposing him to stereotypes and a high rate of racial incarceration. If the Miami district would have put forth the effort and financial resources into creating a CIT program, Baker and other mentally ill “criminals” would not only be alive, but also getting the treatment they deserve.

The complexities that arise when combining multiple target social identities. This graphic demonstrates the statistics on black people with mental illnesses, which predisposes them to potential incarceration based on profiling. Graphic courtesy of Mental Health America.
Dr. Amy C. Watson at the University of Illinois at Chicago and Anjali J. Fulambarker, a Master of Social Work, discuss the research behind the newly implemented program in their article, “The Crisis Intervention Team Model of Police Response to Mental Health Crises: A Primer for Mental Health Practitioners”. Watson and Fulambarker highlight that recent studies show that CIT has improved the safety of first-responder and suspect interactions. In Memphis, there is a correlation between CITs being used and fewer Special Weapons and Tactics (SWAT) teams operating. Additionally, less force usage and fewer injuries have been reported. Watson and Fulambarker found that “CIT officers used force in only 15% of encounters rated as high violence risk and that when they did use force, they generally relied on low-lethality methods. In our study of Chicago’s CIT program, we found that CIT officers used less force as subject resistance increased than officers that were not CIT trained”. Crisis Intervention Teams, such as the one in Memphis, are decreasing police brutality that is based on presumptions, as more thorough analysis of the suspect is completed before making any impulsive, violent decisions. Through an increase in programs like CIT, state officials have the opportunity to change the culture of violence in America. Today, our society is accustomed to treating controversy with brutality, even though we’ve always been taught not to fight fire with fire.
Earley describes why fighting fire with fire is especially hazardous in the mental-health incarceration process. Forcing people with mental illnesses into cell blocks with no treatment before throwing them back out on the street when they are deemed “suitable” is a double-edged sword. It not only makes life miserable for them, but also continues to put others in communities at risk, as the patient often still has delusions and hallucinations that potentially lead to criminal activity. He discloses, “The justice system was completely overwhelmed with mentally ill inmates, and few of them were getting any actual treatment. Instead, they were being shuttled back and forth between the jail and the hospital, being made ‘competent’”. Clearly, the jailing systems of America today are completely reactionary measures, and lack any ability or desire to aid inmates into a smooth transition out of a concrete box and back under the blue sky. This exact dilemma is the reason Crisis Intervention Training programs are long overdue. Prevention is key here, yet many of our institutions are blind to the concept. Or, if they do understand, their vision is far too fogged by politics and money to clearly consider the health of their patients.
As crucial as it is to improve the living conditions and legalities of people who are jailed for their illness, it is equally important–and ultimately preventative–to work on erasing the stigma behind mental illnesses. Watson and Fulambarker note, “Additional research on CIT has shown CIT training is associated with improvements in attitudes and knowledge about mental illness,” as they cite a survey administered to 159 officers before and after 40 hours of CIT training in 2005. After the training, administrators noted a significant decrease in a officers’ aggressive mindsets and an increase in open-mindedness regarding the power of schizophrenia treatment program.
Earley matches this research with a direct quote from Miami Lieutenant Cochran, who reported to Earley that the departments had difficulty talking about mental illness because of the stigma and prejudice portrayed in society. Cochran explains,
“Unfortunately, the police mirror that, and Hollywood magnifies it by always showing mentally ill persons as violent and dangerous and sadistic. When we began CIT training, I began to see these people differently. If you saw a man with a white cane trying to cross a busy street, I can guarantee you that most Americans would help that person cross safely. But every day we pass people who have a mental illness on the street, often they’re ranting, and we don’t see them with our eyes and we sure don’t see them with our hearts. I have a problem with that” (Earley 354).
These new educational programs for law enforcement have the capability to deconstruct stigmas and reorganize how an officer, the first responder before or during any traumatic event, views these victims of their own mental illnesses. Because criminal cases are so heavily represented in our media, society will begin to absorb their attitude change and reflect it into their own behaviors toward the mentally ill.
Crisis Intervention Training programs have the potential to spread change like wildfire, and can absolutely not only decrease the number of non-guilty “criminals” placed behind bars and improve protocol safety, but can also give us all a little more human empathy.
